
Case Study: Chronic Left Sacroiliac Joint Pain

Case Example
Michael teaching a class on the diaphragm.
I have been treating a person with left sacroiliac pain and for many years.
It varies in intensity but is always present. The person is late middle age, active, an avid yoga student, and engaged in life fully. They have good body awareness and yet this pain pattern persists.
These are tricky cases to enter into as I’m not sure what I am going to have to offer since the person has had lots of excellent care before seeing me, has a great yoga teacher and is engaged in an ongoing reflective relationship with themselves and their social world.
Years ago, I learned that research from the NIH was showing that folks with chronic conditions were experiencing "quality of life” improvement without symptom reduction when care provided meaningful connection and cognitive understanding about their situation. So, I thought the least we can do is explore what all might be related to the specific pain pattern.
Listening to the tissues underlies all the work we do. Understanding the body as reflecting and participating within a nested ecosystem that includes natural processes and social contexts becomes part of the “listening field”. This motivates my study of anatomy, fascial concepts, physiology, how mental-emotional and spiritual realities are intertwined with our physical bodies. For those of us who have answered the call to tend to the physical body we return to the body as the ground of inquiry; how does the body experience itself?
The First Few Sessions…
Over our first few sessions together, we established connection through the bodywork and our provider-patient relationship. Their body found the listening based myofascial touch interesting and they enjoyed the opportunity to share where in their body releases would refer to and enjoyed that I was interested in that. We followed their tissues, and sensations, slowly building some frames of reference that related to the SI joint pain.
One of these was the right thoracolumbar junction (TLJ). There was tension from there up the erectors and into the “fascial feathers” (lat, obliques and transversus abdominus). Working here was significantly related to the left SI joint pain.
My myofascial work and anatomy study has taught me that the TLJ is really important - regardless of specific symptom picture. So, I was paying attention to what we were learning together and orienting my curiosity around this right TLJ connection.
Good Sessions, No Symptom Change
But here’s the rub, everything seemed positive in treatment but there wasn’t much symptom change. But, she was learning about her body and felt like we were making “progress”. Which I interpreted to mean that the learning was meaningful and her relationship with the symptoms was shifting even if the symptoms were not.
Clinical effectiveness is what motivates all the work we do around here. Thinking about “results” can be tricky in our work as it can invite ego into the equation in an unhealthy way. However, there is no doubt some form of relief is part of what folks are seeking.
It’s interesting to think about two of the terms above; “clinical effectiveness” and “relief”. Neither explicitly means reducing or eliminating symptoms, though often that is implied. Depending on the nature of the case symptom reduction or elimination may or may not be the most realistic outcome.
A Breakthrough from a Breakdown…
In maybe our 4th session there was a lot of action. We focused on similar areas but things seemed to be extra talkative in their body. We both felt that the system was more responsive and that there was more tissue change happening than in previous visits. When the session ended they felt great…
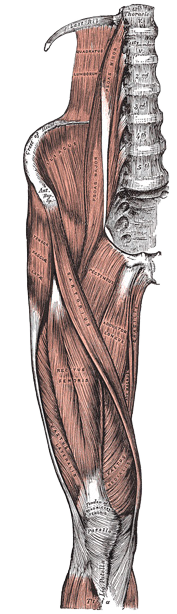
The muscles and fascia of the iliac region
Anatomy of the human body, by Henry Gray. 20th ed., thoroughly rev. and re-edited by Warren H. Lewis.
And then the other shoe dropped. I’m sure you have been there. The patient messaged me that they were in debilitating, acute pain. Hardly able to walk, not able to sit, and in constant pain. Yikes!
One of my clinical processes is to step into these moments with a lot of curiosity. So when the patient reached out to share that they were in acute pain I got them into the clinic asap. It was my admin day, which I was in part spending at urgent care for my own health related issue. I was fine, just concerned about something that I felt needed some diagnostic attention.
The patient and I scheduled for after my urgent care visit, when scheduling I told them we needed to be a bit flexible as I had a doctor’s appt and I wasn’t sure when I was going to be done. I believe in humanizing healthcare which means humanizing the provider too (with good boundaries and skillful intention). I let them know I was having a health issue I needed to tend to but could be available later in the day if they were flexible.
(There is another issue here, that is that lots of us have to go to work when we are struggling in our own bodies.)
They were super grateful I was going to see them right away and also concerned about my well-being. I let them know I was overall fine and happy to be able to see them and find out what was going on. This dynamic actually added depth to our care relationship.
The session that ensued became a breakthrough for the patient and ushered in a very cool treatment dynamic. Chronic or long-standing pain that has an acute flare can be really tricky to treat. We both felt that the previous session had loosened some compensation patterns their system depended on. Without the compensation the left SI joint pain increased significantly and amplified into a larger pain dynamic.
Given the severity of their discomfort, I wasn’t comfortable with them laying face down, so they started face up. I knew the right TLJ was an area of interest and had been part of what had loosened the holding patterns. I started with a diaphragm release that we teach both in our Myofascial Release Series and is the core of our Integrated Visceral Techniques course.
The diaphragm is a major structure of the TLJ and I thought it could potentially offer some relief and also treating it would give me some information on what might be happening and how we might approach it in the moment.
There was an immediate response in the affected area - mostly positive. I was working very gently and very deliberately. From previous sessions, I knew the tension went up the erectors from the right TLJ so I gently palpated along them and offered gentle mfr where I noted tension. We teach something called tension adjacent techniques, find the tension and work along the border of the tensions and not into it. I was doing that. It all seemed interesting to their body. But I wasn't sure where I was going to go with it.
I had not done any visceral work with them and given that the right TLJ is also related with the liver and that we were working right there, I would try some gentle liver techniques. These opened up their system significantly. They felt pain relief in the left SI joint and also noted interesting sensations in their right knee that had been the site of an ACL replacement over 20 years ago!
I worked from the liver into the right abdomen and down the right leg following the most obvious fascial tension patterns, also guided by the patient’s referral sensations.
The session brought up some old emotions for the patient and dropped them into a pretty deep, altered state. When the session ended their pain was down about 50% and they continued to improve after the session.
Clinical effectiveness is obviously what we are all looking for when we go to work. But, thinking about “results” can be tricky as it can invite ego into the equation in an unhealthy way. However, there is no doubt some form of relief is part of what folks are seeking.
It’s interesting to think about two of the terms above; “clinical effectiveness” and “relief”. Neither explicitly means reducing or eliminating symptoms, though often that is implied. Depending on the nature of the case symptom reduction or elimination may or may not be the most realistic outcome.
The Care is the Goal
When they reached out in distress I knew I was going to see them asap, it's just how I always handle those situations. In this instance, my admin day that had also become my own healthcare day, was my best chance. I had no idea what I was going to do or if treatment would alleviate any of their symptoms. But I knew that showing up was the care and being alert and present to the moment would be the best path to a positive outcome, whatever that might be.
One of the main outcomes was a deepening of trust and the patient feeling cared for regardless of symptom change.
Paradoxically, this process led to some symptom change. Maybe it wasn’t even the “work” that created the symptom change but just the “care”.
What’s Come Next Has Been Super Fun!
The patient has also been working with a wonderful PT. I am not super analytical when I work, it takes away from my other skills. I find good PT’s to excel at analyzing and interpreting pain patterns from a biomechanical perspective and offering great tools to patients.
So, when the patient came in after the breakthrough and asked me if I was interested to watch a video she recorded of her PT’s assessment, I said “heck yeah! “ And, it was so cool! We were treating the same dynamic but each of us from within the center of our best skills and our best role for the patient. The PT’s assessment as shared in the video affirmed some things I was thinking and gave me ideas about other areas to explore.
We now also record me at the end of the session sharing what I learned and the patient has that to remind themselves (helping anchor in their cognitive understanding about their body and this chronic pain). The patient shares this with the PT and the three of us are working together as a collaborative team. The patient is super excited about their progress, the insights they are gaining and having a well functioning healthcare team.
The Takeaways
I am so grateful to have a way of working that allows me to be comfortable and curious in these sorts of settings. I don’t think these types of case situations are easy nor are they predictable. Having multiple techniques or lenses to use when I work allows me to explore with a patient’s system in a meaningful way. Because we built a solid relationship prior to this happening we were able to use that to actually further the trust. The patient became even more engaged in treatment and on their own figured out how to include their PT’s wisdom in the treatment room.
Interested in how this translates to real-world practice?
Check out some related articles:


