
The Myodural Bridge
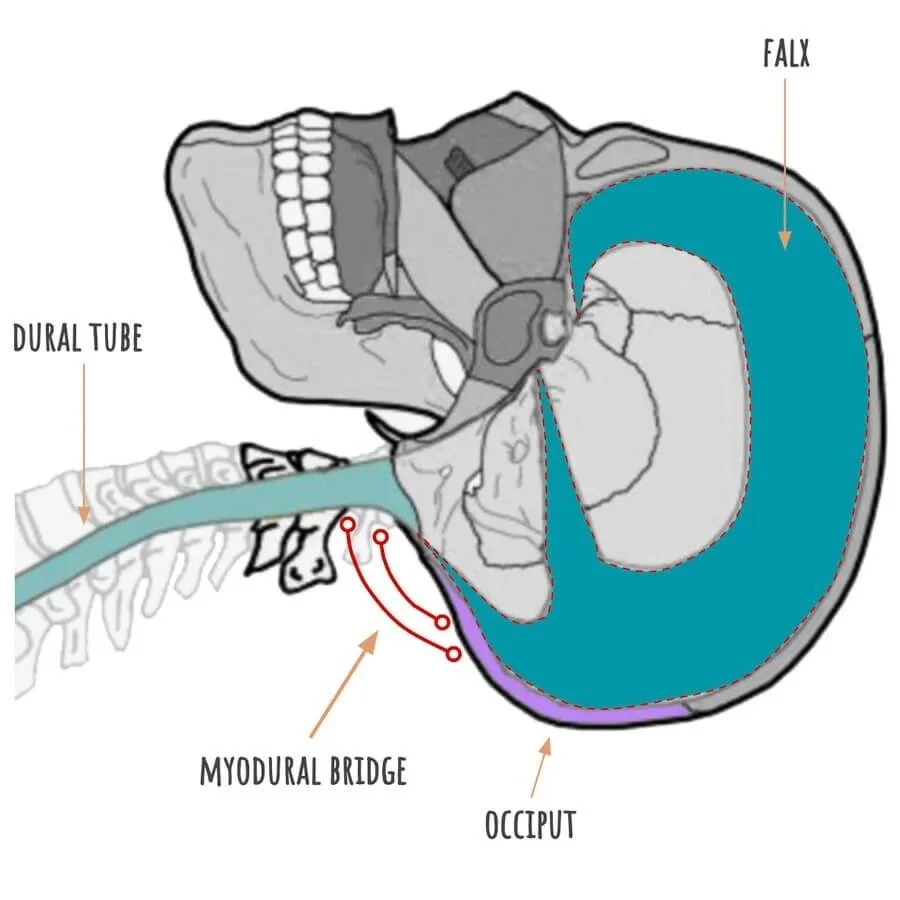
Image: Adapted from Volksmed
The myodural bridge is where myofascia of two of the sub occipital muscles, the rectus capitis posterior major and minor, have fascial connection with the dural tube–the membrane surrounding the spinal cord. This means that good myofascial work at the sub occipitals could also be considered fairly direct work on the craniosacral system.
Let’s unpack the anatomy a little more and explore why and how working here can impact so many symptom pictures and feel so satisfying to the person receiving the work.
Sub Occipitals Anatomy Overview
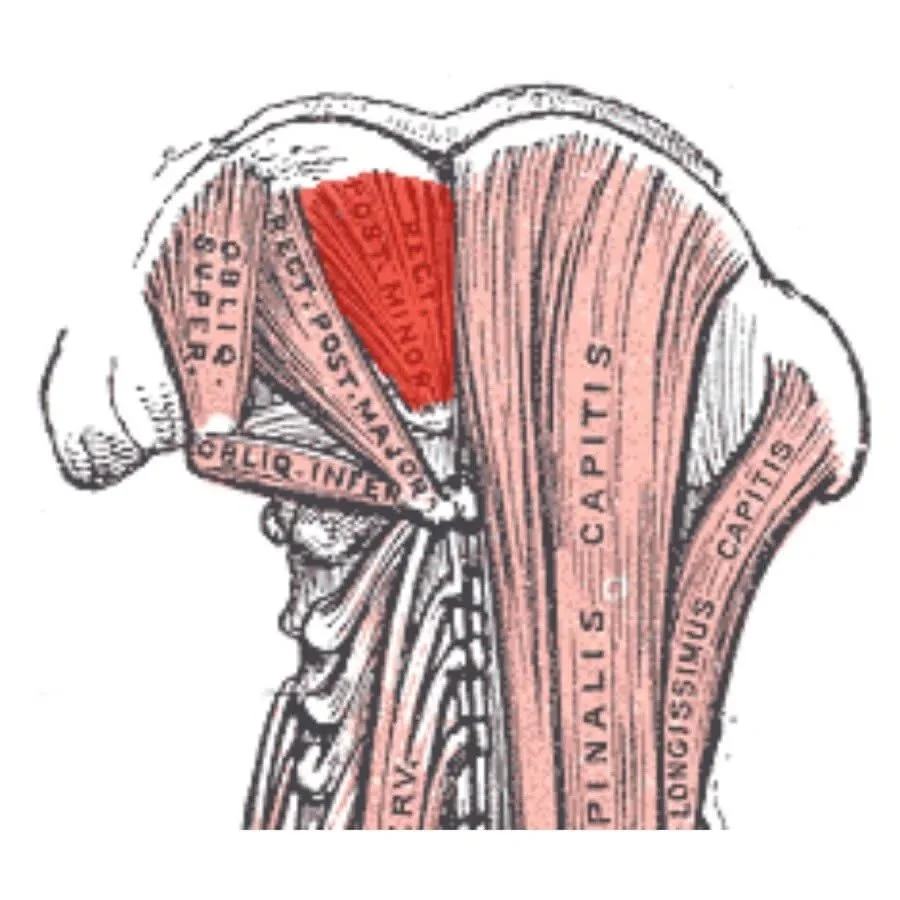
Image: Suboccipital Muscles (Gray)
Let’s start with the sub-occipitals, specifically the rectus capitis posterior major and minor. These are deep to the rest of the cervical myofascia, and they attach to the occiput at the inferior nuchal line (the lowest bumpy ridge on the back of the head). These muscles are very close to the midline, with minor being the most medial, on either side of the midline and attaching to the spinous process of C1 (you could consider these midline structures). This means they are short and almost vertical. Rectus capitis posterior major is just lateral to minor on the occiput and goes to the spinous process of C2. They are a bit longer and only slightly more lateral.
The atlanto-occipital junction + C2 is an area of profound tension in many people. On dissection, the fibers of the rectus capitis posterior major and minor are sometimes so dense as to appear more like tendons or ligaments. The spaces are small, the movements minute, and if tensions arise they can become fixed. These two muscles can play an outsized role in compressing the occiput onto C1 and the both of them onto C2. Later we will look at how this potentially impacts arterial flow into the brain.
Sub Occipitals, the Foramen Magnum (the transition from intracranial to extracranial space), and the Dura
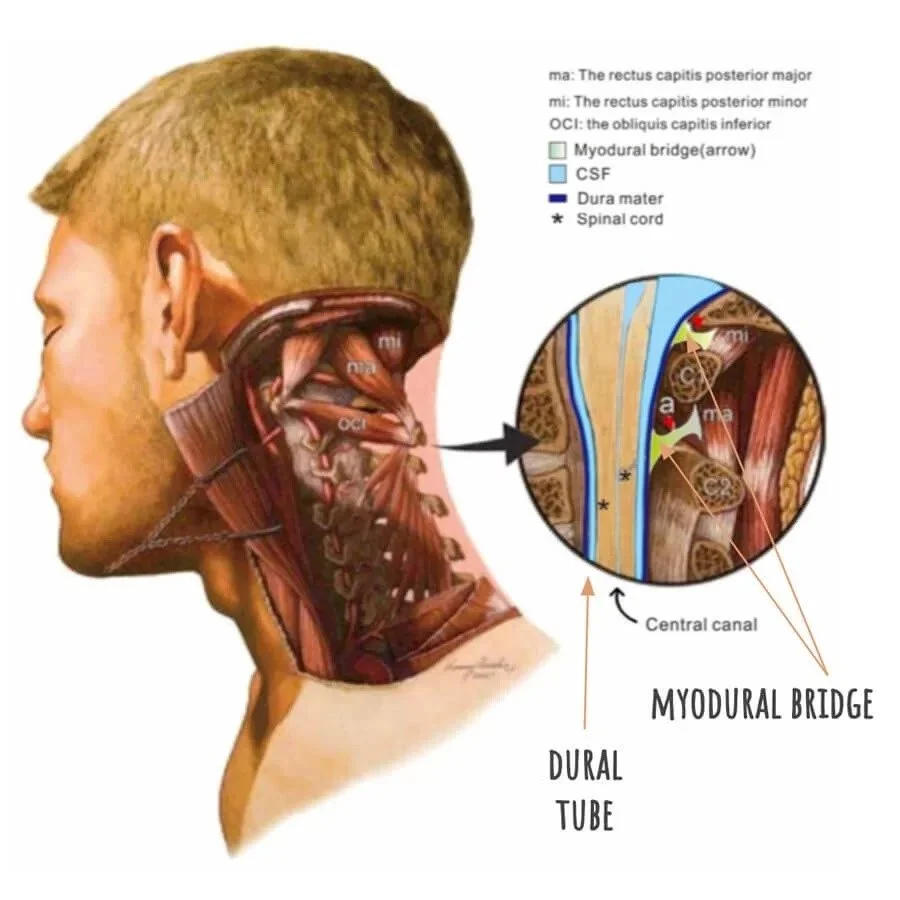
Image: Myodural Bridge (Scali and Quirk)
In addition to the anatomy just discussed, these two muscles have an added attachment to the dural tube just after it exits the foramen magnum. The foramen magnum is the hole at the bottom of the occiput and serves as the transition from the brain stem to the spinal cord, from intracranial space to extracranial space, inside the cranium to outside the cranium.
The dural tube is the fascia that surrounds the spinal cord and contains the cerebrospinal fluid as it flows and bathes the spinal cord. The membrane is contiguous like the membrane system within the cranium.
The foramen magnum is in close proximity to the rectus capitis posterior minor and major occipital attachments. We can imagine a fascial weave at the foramen magnum that is a combination of dural tissue, connective tissue from a combination of the ligaments around the atlanto-occipital junction, and the rectus capitus posterior minor and major. When there is significant tension in these extracranial tissues it will impact the craniosacral system.
Tension here potentially–and in ways that might not be measurable with technology yet still be important to the body–constricts the space at the foramen magnum. Even a subtle constriction here can impact fluid flow from the intracranial to extracranial spaces.
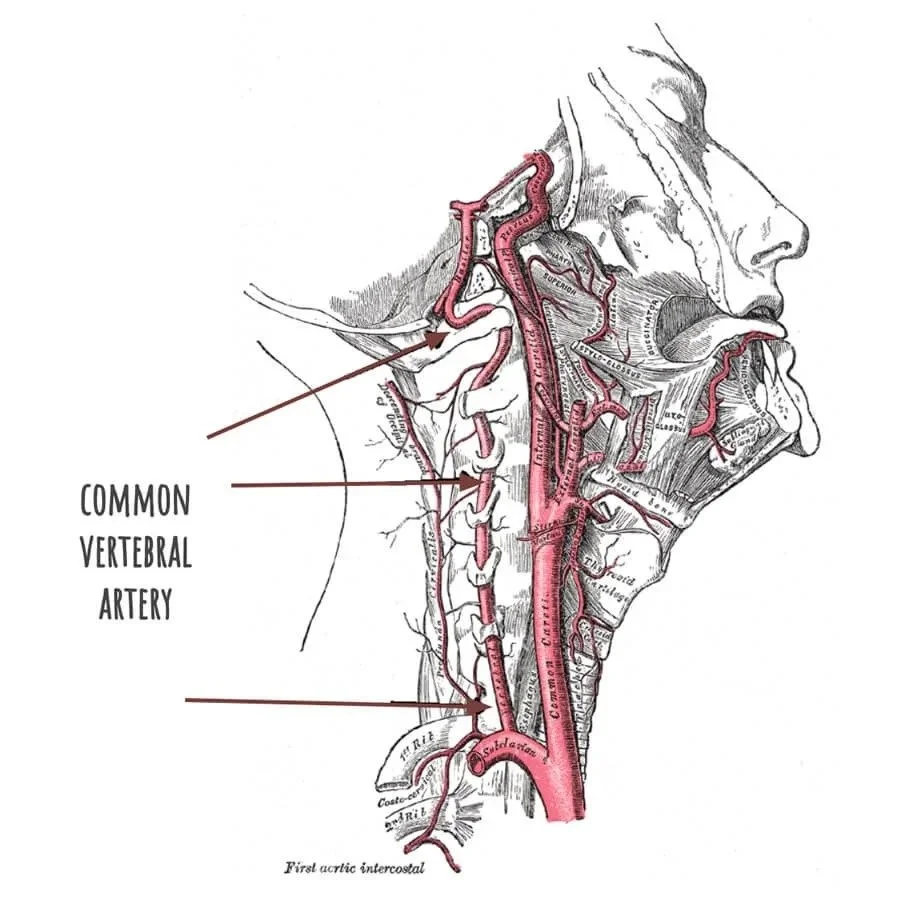
Image: Common Vertebral Artery and Internal Carotid Arteries (Gray)
This area is one place where the “glymph”is thought to leave the cranium and enter the lymphatic system. Glymph is a blending of fluids from the glial cells and the lymphatic system. This fluid flow is now being considered as an important component of our immune system, especially providing immunity to the CNS.
Arterial Blood Flow to the Head
While not directly related to the myodural bridge, compression at the occiput, C1 and C2 can also impact blood flow through the internal carotid and common vertebral arteries. The common vertebral artery makes two sharp turns as it passes these vertebral levels and compression or any vertebral deviation or rotation here potentially impedes blood flow and thus oxygen to the brain. The internal carotid artery rests along the anterior surface of each side of the cervical vertebrae beginning around C3 or 4 and passes into the skull through a foramen (little hole) in the petrous portion of the temporal bone, the carotid canal.
This is relevant in so many clinical presentations. Often head injuries and post concussion syndromes also have related neck issues. Significant neck and shoulder tension over time can adjust posture and vertebral position such that low grade yet noticeable to the body congestion occurs here. This can result in symptomology that might be considered “subclinical” within conventional medicine. But, just cause they can’t see it or measure it doesn’t mean it isn’t happening. It just means that technology has limitations (gasp!).
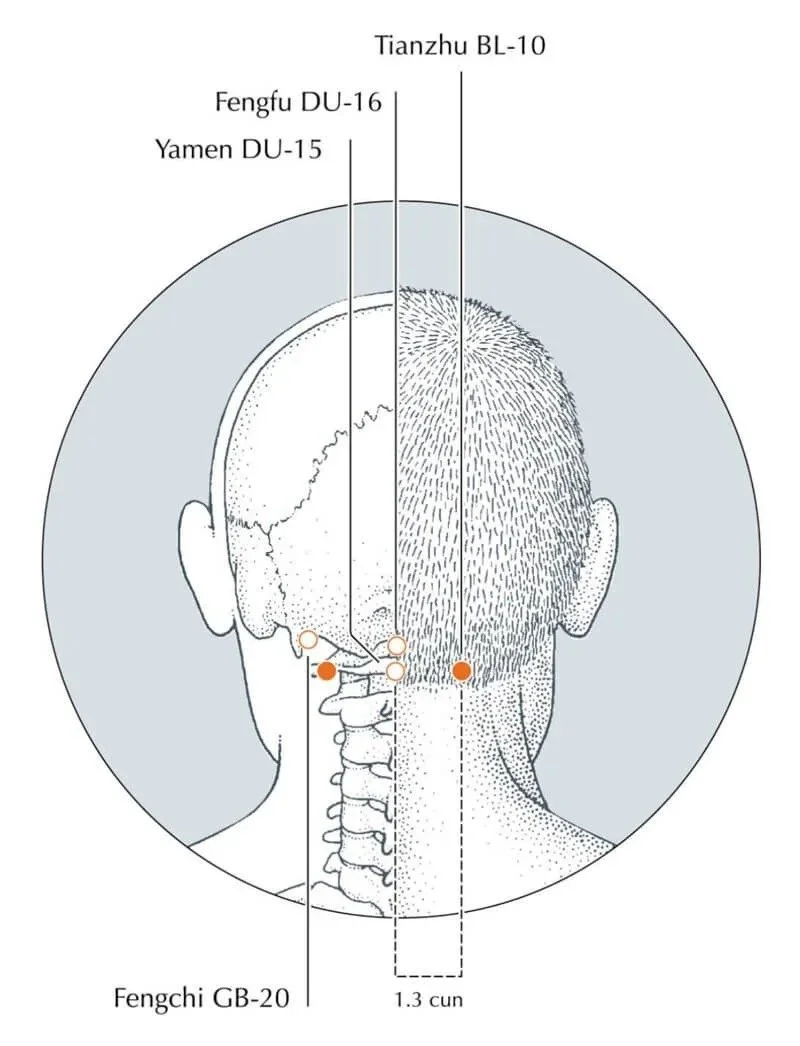
Image: Bladder-10 (Deadman, a Manual of Acupuncture)
East Asian Medicine Perspective
In the East Asian medical system the acupuncture point that goes with the myodural bridge is bladder 10, Tian Zhu or the Great Pillar. It is part of a special category of points called Celestial Windows or Windows to the Sky or Windows to Heaven. As a group they specifically treat disharmony between the qi of the body and head.
How many times a week or a month do you have a client or patient who is dealing with brain fog, mental fatigue, racing thoughts, etc. All of these symptoms have myriad causes: post covid-sequelae, post-concussion sequelae, digestive system related headaches and brain fog, tension headaches, etc… We could go on and on. Each of these could be said to reflect a disharmony between the body and the brain.
When an acupuncture point is within a special category, often we find some interesting anatomy that helps us understand the region and its importance to the body. This is not to reduce the potency of East Asian medicine to anatomy, but we should be curious about what is being signified and to see if we can learn more about how the body experiences itself by combining curiosity with different models of the body.
Takin it to the Streets…
I imagine most of you do some work in this space already. I hope diving into this anatomy inspires you to spend more time there, work more slowly and deliberately, and give the body some time to unfurl itself in response to your presence. Even if you have not yet studied CST you will be impacting that part of the body by working here. If CST is part of your practice but you have not learned this anatomy in your studies, I hope this offers you some confidence to see this work as an opportunity to deepen your CST approach. And of course, to all my acupuncture colleagues, it is so fun to add more understanding to the ecology of the points.
Remember, our work is part study and part theory building by actually being with the body in real time on our tables. No book can cover everything we will experience. The body is the book.