
Entering the Temple of the Jaw
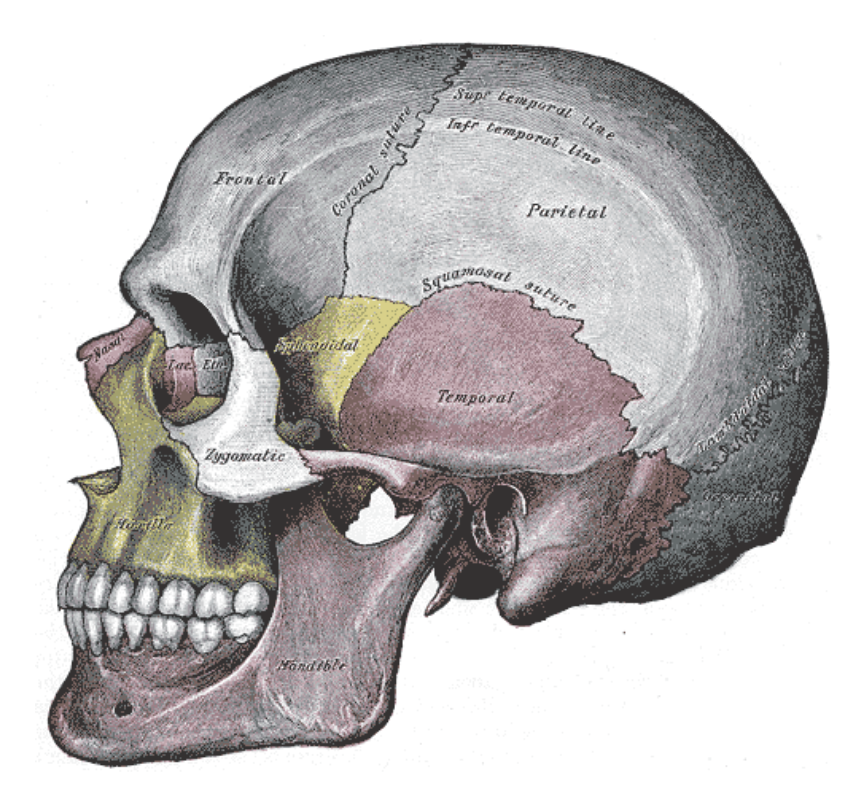
Image: Gray
When in doubt, check the jaw. In our mapping of the craniosacral system, I place utmost importance on treating the jaw. While not directly part of the CS system, the jaw may be the place where the most energy enters into the system. I want to share a case study as an example of how this can work in the clinic.
Acute Presentation in a Chronic Pattern
I have been working with this patient for a couple years now. They have a severe TBI (traumatic brain injury) that has left them unable to work, struggling with balance/gait issues, aphasia (speech difficulty), sensitivity to sound, and fatigue (both physical and cognitive). These symptoms are variable in severity yet all are persistent. Over the course of our time working together (doing primarily CST and MFR) all of her symptoms have improved but she continues to experience episodes of significant symptom expression.
The patient came in last week unable to stand upright–she was tilted to the right and hunched over. The aphasia was noticeably worse. She had been having a very difficult time and was mostly bed ridden for the previous few days. This episode made sense as she had recently travelled and done a ton of work prepping a home for sale amidst an intense heat wave and with no AC. Any one of these factors would likely lead to an increase in her symptom expression.
Trust in Treatment
I know the patterns in this person’s system from our time spent together. I know what usually offers relief, knowledge I have going into this session. For this person, they experienced a heavy impact on the left side of their face/jaw and fell, and we hypothesize that they then hit the right side of their head on something. They don’t have memory of aspects of the experience.
Her major symptoms are on the right side, mainly temporal bone and behind the eye. She experiences intense pressure in and behind the right eye, a muffled sensation in both ears but worse in the right, and additionally a tight band around their head, with more tension on the right side.
In this session their system was on high alert, all the tissues were under more pressure than is typical, so I started with a lighter hand than usual and I chose to work away from those main areas of symptomology. After gentle cervical myofascial work to assess and offer some treatment, I began doing very gentle releases around the TMJ, focusing on the mandible, not the temporal bones.
The body responded well to the work on the jaw and so that became a main focus of the treatment. My understanding of the relationship of the jaw with both the cranial and myofascial systems allowed me to sink into the work I was doing and trust it would be helpful. We danced with the mandible, cervical myofascial work and then lightly, intermittently added the main cranial releases. I was imagining titrating the inputs into the system, checking for the system’s tolerance through tissue response. Slow, methodical, with specific curiosities about how the body was responding to the work and being willing to change and adjust my work based on interpreting the body’s responses.
I added in work with some facial bones (zygoma and maxilla) and continued dancing with the jaw and temporal bones (and of course checking in with others, but decompressing the TMJ was my main focus). Over time, the pressure in the eye released and the band around the head loosened. These are indicators in the session that we are doing well. With the system starting to release its tension, I was able to enter into treating the rest of the pattern in her system, further integrating it into the cervical region offering decrease in tension there as well. We did some grounding via the sacrum and the dural tube towards the end of treatment, complimented by dural traction via the parietal bones.
As I walked her to her ride (she doesn’t drive so her husband was there waiting for her), we both noted that she was standing totally upright, the right-forward lean was gone. Her gait was still wobbly. Her brain fog was much better and there was very little if any pain.
AN ASIDE
One thing we rarely discuss in our field is the pressure of situations like this. It happens regularly; someone is suffering from an experience with/in their body-mind and has chosen us to offer them potential relief. Of course, we want them to have that relief, I think both from our genuine desire to help and the natural expression of our ego (which it is our job to constantly be working with so that it is less/non intrusive in these situations).
I rely on two things in these moments. One is just experience. I have been practicing a long time and have had ample opportunity to come into relationship with this practice dynamic. I let myself feel into the moment, feel their struggle or suffering, try to appreciate its impact on them and the specific dynamics of their life. This comes from Bonnie Badenoch’s teachings. We can embrace our experience in the treatment room and use it to build connection. All of this depends on us having our shit together, so to speak, so that we don’t merge with them and their experience. This is why I advocate for each of us being engaged in some process whereby we are cultivating awareness around our own issues so that they are not seeking engagement in the treatment room.
Secondly, is my relationship with the principles that underlie the work that I do. There really is one principle with two parts. The principle is Trust. I learned in my first ever bodywork training, a CST course of all things, that one of the osteopathic principles is trusting the wisdom of the body. How can we then participate most meaningfully with that wisdom? That is the singular question I’ve been asking in my clinical work, my study, and my teaching.
This is why I love relational anatomy study: because it amplifies my relationship with the tissue-verse. Understanding the relationships between tissues and the properties created by the betweenness offers me specific and tangible processes to trust. Trust fundamentally implies relationship/s. So, what aspects of your work are you in relationship with and how can you amplify that connection and deepen your trust in it?
This is why I view all our courses as opportunities to find apprenticeship with the body itself. There is no better teacher.
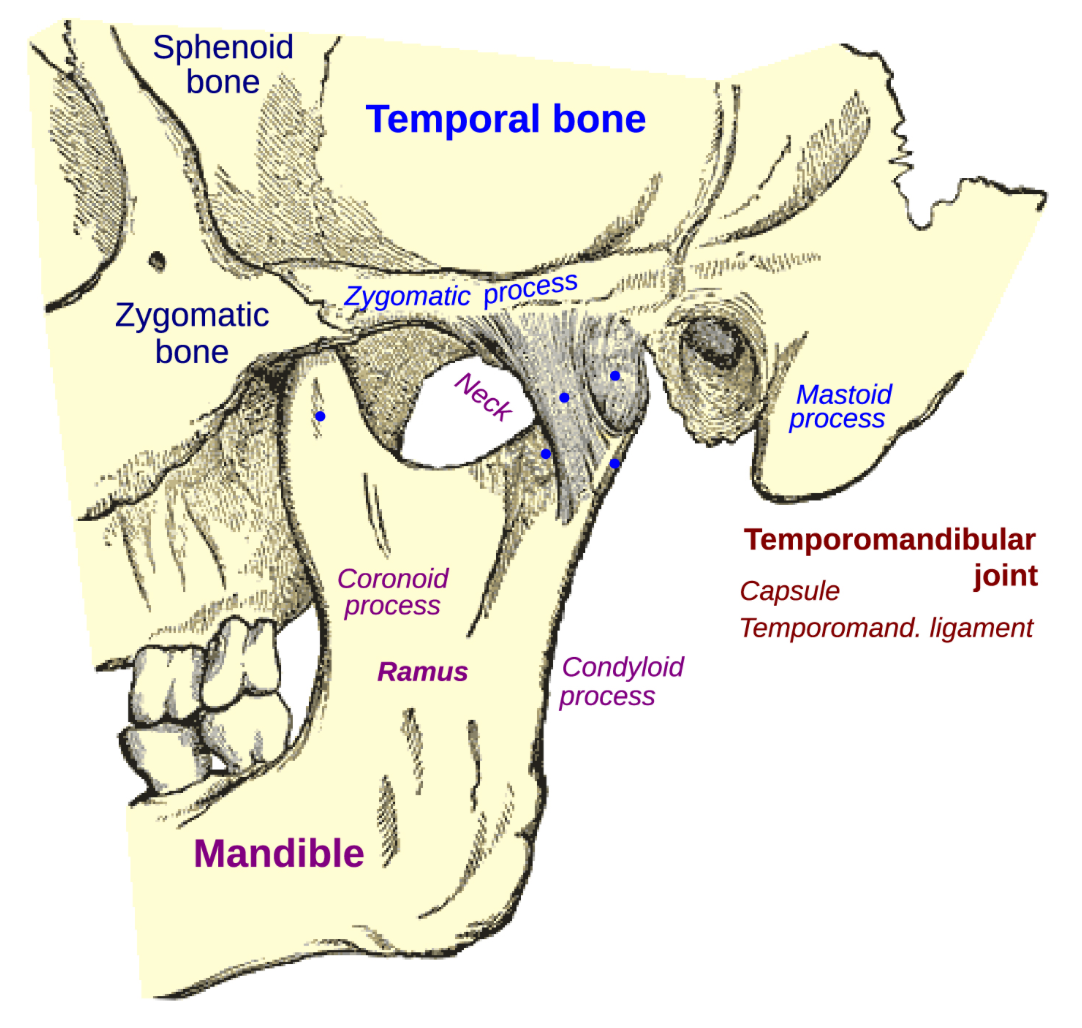
Image: Gray
Some Takeaways
Of course, we do not always or even often get these results. This was an acute flare up of a chronic pattern. Acute flares are often amenable to more dramatic relief. The longer standing patterns change much more slowly. I was aided by my relationship with this person and their system, and my relationship with my work. This allowed me to sink into the moment with her and move slowly, with curiosity and patience, following the wisdom of her body and my understanding of relationships between the different tissues.
The thing about trust is that it builds over time and is something that we can cultivate. I have found that the combination of study and reflecting on my clinical experiences is the surest way to build trust, not in myself, but in the work that occurs in the space between me and another person and their body.